


Frequently asked questions
This section is dedicated to answering the most frequently asked questions we receive from our patients about cosmetic procedures performed in our clinic.
What are the advantages of the endoscopically assisted axilla technique?
The advantages of the TEBA, endoscopic transaxillary technique are:
- NO breast scars; the scar is located in a fold at the top of the armpit, making it difficult to see even with arms raised, even to an experienced eye Consider that scars are FOR LIFE! They cannot be erased by laser or any other surgical or medical technique, so once done they will be PERMANENT. For this reason, it is very important that the scar is hidden in a fold under the arm, away from the breasts. For example, when you lie on your back, the scar is not visible (because there is no scar on your breasts), but this is not the same when the scar is present under your breasts, it stands out even more. In the armpit the scar is hidden in a fold, so it is very hard to detect and does not attract the eye. The scar located in a fold at the top of the armpit always heals much better than in other areas because the area is mobile and folded, where the scar can easily be hidden.
- The precision with which the operation is performed is much greater than in traditional surgery under the breasts, as the operation is visualized on a monitor that enlarges the operating field approximately 10 times, similar to robotic surgery. So what we actually see as 1cm , on the monitor is magnified to 10cm , so we can say it has a millimetric precision (1mm in reality is magnified to 10mm on the screen)
- It is a minimal invasive and atraumatic surgery , the intervention being done from a distance, under maximum control, endoscopically, with special atraumatic devices, similar used in robotic surgery
- In the long term, there is much better stability of the implant as there is no damaging or altering of the inframammary groove ligament, as there is with the under-breast technique.
- Dissection is performed using state-of-the-art nanotechnology instruments, similar to atraumatic robotic surgery, so recovery is much faster and safer, reducing operating time and hospitalization.
- In special cases of moderate mammary ptosis, it can be done internal lift , by internal suspension of the mammary gland , so avoiding classical scars used in mastopexy – breast uplift
- In special cases of moderate tuberous breast, we may use TEBA to correct breast malformation by internal manipulation of the mammary gland through the armpit, thus avoiding scars on the breast
- The risk of the scar dehiscence with the exposure or exit of the implant, that is present with the under-breast technique due to the tension (pressure) created by the breast implant at the breast level, is practically non-existent with the TEBA transaxillary technique, as there is no tension (pressure) in the armpit, which is present in the breast.
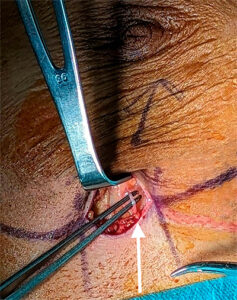
- The risk of loss of nipple sensitivity and breast skin from the nipple down to the inframammary fold is much reduced as the scar is placed away from the breast, under the arm. The intercostal nerve is not sectioned, as it often passes through inframammary fold, as seen in the picture bellow and indicated by the white arrow. In case that this nerved is damaged, you may lose nipple sensation and skin bellow the nipple sensation down to inframammary fold.
- Any kind of bra can be worn, including those with braces (whalebones), as they do not press or embarrass the scar (as can happen when the scar is under the breast).
- The implant can be positioned either in front or behind the pectoralis muscle. If you later wish to change the implant for a larger or smaller one, the procedure can be performed through the same scar under the arm.
- There is no risk of deforming the lower pole of the breast as can happen in some cases due to scarring under the breasts which can alter the appearance of the breasts at the bottom (scar retraction).
- The nodes under the arm, the sentinel node and the nerves under the arm are not affected
- The risk of infection is not increased by any means by transaxillary approach compared with classic technique under the breast
- Today, endoscopic-assisted underarm breast implantation is the most advanced breast augmentation technique using state-of-the-art technology in the field. This procedure is our main recommendation and today we are considered one of the world leaders in this field.
WHAT IS THE PROCEDURE ITSELF?
Breast implants are placed either in front of or behind the pectoral muscle through a minimal incision of about 3 cm placed in a crease at the top of the axilla. At the time of healing, the scar is hardly detectable, as it is perfectly hidden in the fold in the armpit. The implants are placed using an endoscope (in popular terms also known as a 'laser') connected to a monitor, in 3D, which allows the surgeon to visualize the operating field and the design with maximum precision and clarity, up to 10 times image magnification. That means that what we see in reality of a size of 1cm, on the screen appears of 10cm. So the surgery is performed with a much higher precision than clasic technique.
WHY IS THIS INCISION (CUT) CHOSEN BY PATIENTS FOR BREAST IMPLANT?
Many patients prefer this type of incision because it is the only way to avoid scars on the breast and to avoid cutting the breast tissue when placing the implant. Normally, the scar under the arm heals extremely well and is barely detectable. So, first of all, NO BREAST SCARS! Other advantages are that the accuracy with which the procedure is performed is greater, as it is performed on a monitor that increases the operating field by approximately 10 times. Special nanotechnology instruments are used, the most atraumatic and similar to robotic surgery. Recovery is faster and the risk of loss of sensitivity or numbness of the nipple and skin breast is much lower than with the traditional technique. On top of that, the risk of the implant coming out or being exposed through the cut under the breasts (existing with the classic technique under the breasts) is practically ZERO! In the case of cutting under the breast, due to the high pressure on the scar, sometimes the scar can open and the implant can be exposed through the cut made under the breast.
IS IT MORE DIFFICULT TO PLACE IMPLANTS THROUGH THE ARMPIT?
In fact, it's easier for a surgeon trained in this operation. The dissection is done under direct endoscope control, 3D monitor viewing and magnification up to 10 times of the operating field with maximum precision. The breast tissue is lifted without being sectioned and the implants are placed precisely in the correct position with millimetric precision.
IS THIS AXILLARY APPROACH TECHNIQUE MORE PAINFUL?
Under no circumstances. Although each person's sensitivity threshold varies quite a bit, generally following this procedure there is a pressure, muscle fever-like discomfort that is felt for the first few days, but which eases slightly when pain killers are taken. Recovery is usually quicker with this technique, as the incision is placed at a distance from the surgical site and the operation is performed using special atraumatic nanotechnology instruments, similar to robotic surgery.
CAN THE IMPLANT BE PLACED ABOVE AND BELLOW THE PECTORALIS MUSCLE?
Of course, with equal precision the implant can be placed either behind the mammary gland or behind the pectoral major muscle fascia or even behind the pectoralis major , including the "dual plane" techniques as type 1, type 2 or type 3.
IS THERE A HIGHER RISK OF INFECTION?
No, no way! Studies have shown that the risk of infection is the same regardless of where the incision (cut) is placed and very low. As a result, there is no increased risk of infection with this procedure.
WHAT CARE IS NEEDED AFTER THIS TYPE OF SURGERY?
Care is very simple. You can shower daily, then apply Betadine and an antibiotic ointment (Baneocin). The sutures dissolve on their own and do not need to be removed. The arms can be raised above the head.
HOW DOES THE INCISION UNDER THE ARM HEAL? AND HOW WILL IT LOOK AFTER HEALING?

1. Hypertrophic scars under the breast |

2. Keloid scar at breast level |

3. Scar is 3 cm long in a crease at the top of the armpit undetectable |

4. Scar in the armpit at 1 year postop |
WHAT HAPPENS IF A REOPERATION TO ADJUST/ CHANGE IMPLANTS IS NEEDED IN THE FUTURE?
If in the future a second implant adjustment or replacement, or correction of a capsular contracture, is needed, this can be done through the initial incision made under the arm. Only in rare or severe cases may a separate breast incision be necessary.
HOW ARE THE RESULTS LIKE WITH IMPLANTS INSERTED ENDOSCOPICALLY THROUGH THE ARMPIT?
In our practice, we can say that the results obtained with this technique are really excellent, thus results obtained with TEBA are, of course, above the results obtained with the classic technique with scar placed under the breast. The patients are extremely satisfied with the results and the fact that they do not have any scars on their breasts (see our patient references).
IF THE IMPLANT IS INSERTED WITH SCAR UNDER THE BREAST, IN THE INFRAMAMMARY FOLD, IS THE SCAR MORE VISIBLE?
Although we are the first to report reducing the scarring under the breasts to just 3 cm, in some cases the scarring becomes visible and sometimes even disturbing. It can stand out when the patient lies on her back in bed or if she wants to sunbath topless or if the bra raises a bit above the inframammary fold, the scar will be pretty visible.
But with placing the scar in a fold at the top of the armpit, there are very good chances that nobody knows that you have breast implants, thus avoiding a potential unpleasant situation.
WILL I BE ABLE TO BREASTFEED AFTER THIS KIND OF INTERVENTION?
With this technique, we practically do not touch the mammary gland, and the milk ducts (which carry milk to the nipple) are not cut. So, this technique does not influence the milk function in any way. We have had countless cases where patients have breastfed after this technique without any problems, even after several pregnancies.
ARE THERE MORE THAN ONE TECHNIQUE WITH TRANSAXILLARY APPROACH?
Yes, there are several techniques using the transaxillary approach (the axillary region being quite large). With TEBA technique that we use, the scar is placed in a fold at the top of the armpit (blue line in the image), so that it is invisible when the arm is placed at the side of the body. Also, with the TEBA technique, the implant can be positioned behind the mammary gland, behind the pectoralis muscle fascia or behind the pectoralis muscle, including performing all types of "dual plane" technique: type 1, type 2 or type 3.
In other cases of the transaxillary approach, in which the dissection is done with a balloon, the scar is placed on the edge of the pectoralis muscle, so that when you place your arms at the side of the body, part of the scar is visible, not hidden. Also, with the balloon technique, the implant can only be positioned behind the mammary gland, and the dissection is done "blindly", being not even close as precise or as safe as with the TEBA technique. With the balloon technique, or blind dissection, only a certain type of implant can be inserted, injectable (that is not FDA approved), while with the TEBA technique, any type of implant can be inserted, from any company, including all those approved by the FDA (Food and Drug Administration) in the USA or CE approved in Europe.
In the images below, you can see the difference, related to the placement of the scar in the armpit between the 2 techniques. It is worth mentioning that scars heal much better if they are placed in a crease of the skin, as it is the case with TEBA or in the case of upper blepharoplasty, where the scars heal much better than in other areas of the skin, being practically invisible.

 |
 |
|
|
| 3 cm scar hidden in a fold under the arm (via TEBA) Scar under the arm at 1 year, practically invisible | |
WHICH PLASTIC SURGEONS PRACTICE THIS TECHNIQUE?
Not every plastic surgeon practices this underarm approach technique. Currently less than 1% of plastic surgeons practice this technique. Endoscopic axillary implant insertion requires special training and expertise on the part of the surgeon in addition to normal training. Your plastic surgeon should have very good experience with all implant insertion techniques, either under the arm (through the armpit), under the breast or periareolar (around the nipple), to give you the best options and the best choice for your particular case. Intruducerea implantului prin axila endoscopic necesita pregatire speciala si expertiza din partea chirurgului, suplimentara fata de pregatirea normala. Chirurgul d-voastra plastician ar trebui sa aiba o foarte buna experienta cu toate tehnicile de introducere a implantului, fie pe sub brat (prin axila), fie pe sub san, fie periareolar (in jurul sfarcului), si de asemenea, o foarte buna experienta cu toate tehnicile de pozitionare ale implantului mamar, fie in spatele glandei mamare, fie in spatele fasciei musculare , fie in spatele muschiului pectoral, inlusiv toate tehnicile « dual plane » tip 1, tip 2 sau tip 3, pentru a va oferi cele mai bune optiuni si cea mai buna alegere in cazul d-voastra particular.
Dr. Porumb Șerban has a great experience with all techniques, including transaxillary endoscopic, which he learned and practiced in America (USA) since 2002, being the first to introduce in Romania the full HD transaxillary endoscopic technique. But of course, over the past 22 years, Dr Porumb improved his technique, now having his own best technique, being invited to hold conference about his technique, to one of the best shows of cosmetic surgery in Las Vegas, USA, back in 2023, when he presented his conference entitled “TEBA- the future of breast augmentation”, that was really well appreciated. He also holds a master's degree from the University of Paris XI (France), under the auspices of the Gustave Roussy Institute, entitled "Surgical Techniques in Carcinological and Reconstructive Breast Surgery", having a complete and complex experience in breast surgery. De asemenea are un masterat efectuat la Paris la Universitatea Paris XI, sub egida Institutului Gustave Roussi, intitulat “Tehnici Chirurgicale in Chirurgia Sanului Carcinologica si Reparatorie”, avand o experienta completa in chirurgia sanului.
DOES DR SERBAN PORUMB PRACTICE THE INFRAMAMMARY APPROACH AS WELL?
Of course he does! The inframammary technique is the most basic and simplest, so it's like asking a Formula 1 driver if he can drive on the road. Even more than that, Dr. Serban PORUMB was the first to report the scar of only 3 cm in length, under the breasts, at the ISAPS congress in San Francisco, California, USA, back in 2010!
Even if I don't have anything inside my nose, why is my nose stuffy?
La ce să te aștepți după operația de Rinoplastie
- Stuffy nose - It is normal after rhinoplasty surgery for the nose to be stuffy due to post-operative oedema (swelling), which occurs both on the outside and inside of the nose. However, the swelling will gradually disappear over time.
- Secretions - In a day the nose normally secretes about 230 ml of mucus that runs down the throat without us being aware of it. After a nose job, due to the sensation of a stuffy nose, you may become aware of this normal discharge. You do not need to worry because of this. The combination of "normal mucus drainage" and "oedema-swelling inside the nose" may cause the drainage of secreted mucus to be on the nostrils and not posterior to the throat.
- Headaches - Unfortunately, headaches are common after general anaesthesia and surgery. Please take only the painkillers prescribed by your doctor, and if necessary you may also be prescribed medication to improve your sleep.
- Strange or unpleasant smell - A few weeks after surgery, you may notice a strange or unpleasant smell inside your nose as a result of mucus buildup inside. This is due to the reduced mobility of the "mucous blanket" inside the nose. As mentioned above, the nose secretes about 230 ml of mucus per day, which is pushed back by the mucus cells. After surgery, it will take between 4 and 6 weeks for the physiology of the nose to return to normal. During this period, you can clean the nasal mucosa by flushing with saline.
- Bruises and swelling - Typically, swelling (oedema) and bruising peaks two days postoperatively. The good news is that a week after surgery, when the splint is removed, they will be much reduced so you can resume your social life.
- Weaker smell - it is normal in the first week when you have the splints in your nose to smell weaker. It will return after the splints are removed, and so will the taste, as there is a connection between the two senses.
- Swollen or numb upper lip- if your upper lip also swells a little and feels a little numb, this is normal after septoplasty. These symptoms are normal and will generally go away gradually in about 2-3 weeks after the procedure.
Why do I feel something leaking down my throat?
Why do I have a discharge from my nostrils in the first days after surgery?
I have a slight headache and can't sleep, is this normal, what medication can I take?
It's been 2 days since the surgery, why has the swelling and bruising increased?
When can I wash my hair?
Can I clean the edges of my nostrils?
Why do I occasionally get a strange smell inside my nose?
It's been 6 weeks since the surgery, why does the nose still swell periodically?
When can you resume flying?
Is it normal for the skin of the nose to be numb?
Is it normal for my upper lip to be numb, swollen and even hurt my teeth?
Daca vi se umfla un pic si buza superioara si o simtiti un pic amortita , e ceva normal dupa interventia de septoplastie. Aceste simptome vor disparea in general progresiv in aproximativ 2-3 saptamani dupa interventie. Deci aceste simptome sunt normale si vor disparea progresiv.
Is it normal that I can't smell and the taste is gone?
Yes, it's normal in the first week when you have the splints on your nose. Smell will return after the splints are removed, and taste will return as there is a connection between the two senses. that I can't smell and the taste is gone?
Severe headache, fever, confusion, neurological symptoms
If you have questions or medical issues that have not been addressed above, it is important not to make decisions on your own. Please contact us by phone if you have any questions or schedule a specialist consultation with your doctor to get the right answers for your problem.
Do not hesitate to contact us:
EMAIL: office@estetis-clinic.ro
TELEPHONE: +40 723 178 801 (from monday to friday)